

When should we stop resuscitating?
This is always complicated. Every case is different, and it’s difficult to pick out which patients in cardiac arrest are likely to have a poor outcome... And what even is a poor outcome? How neurologically injured does a cardiac arrest survivor need to be for it to be considered poor? Patients, relatives, clinicians, and wider society are likely to all have different opinions on this.
The European Resus Council Guidelines (which the UK-based Resus Council Guidelines are based on) are quite helpful. A crucial principle is not to base a decision to stop resuscitation on a single intra-arrest clinical feature.
“Examples of factors that should not be used alone include initial lactate value, end-tidal CO2, cardiac standstill on ultrasound, pupillary response/size, temperature, co-morbid status, no-flow time, low-flow time, and absence of ROSC.”
It is the accumulation of multiple unfavourable indicators that should inform the team decision to stop.
Intra-arrest thrombolysis
If you're going to give intra-arrest thrombolysis, it’s crucial to do it early.
Of course it always takes time to reach the decision (and obviously it's not a benign intervention) but once you’ve decided, a good game is a fast game. Thrombolytics can take ages to work, especially in poorly perfused pulmonary vasculature. The ERC/Resus Council guidelines say to “consider CPR for 60–90 minutes after administration of thrombolytic drugs”. So if alteplase is given late in the resuscitation you're potentially committing to a very prolonged low-flow state. This reduces th chance of ROSC, and significantly increases the risk of irreversible hypoperfusion injury (including hypoxic brain injury).
Annoyingly there is no stated recommendation from the ERC/Resus Council on how quickly the drug should be given in context of a cardiac arrest. Consensus among my colleagues is <15 minutes. Any reader who can cite some decent evidence to support this please share in the comments…
STEMI and intra-arrest thrombolysis
If STEMI (or “occlusion MI”) is the cause of cardiac arrest, primary PCI is the gold standard. As my department is in London, we should be pushing for transfer out to the cath lab if there is a diagnostic certainty and positive prognostic indicators – such as getting ROSC, good physiological reserve, ETCO2 persistently >1.33 kPa and trending upward, reactive pupils, reasonable acid-base etc.
However, when there is diagnostic uncertainty (STEMI vs PE) intra-arrest thrombolysis may be the most pragmatic option.
New RBBB
New RBBB as an ECG finding in the context of a patient presenting with chest pain or, indeed, cardiac arrest is always a big deal. RBBB doesn’t get the same attention as LBBB... and it arguably should.
The right bundle runs down the the interventricular septum (along with the left anterior and left posterior fascicles of the left bundle) which gets most of its blood supply from the LAD.
Therefore, new RBBB in the context of cardiac-sounding chest pain is suggestive of coronary artery occlusion. If the new RBBB is combined with LAFB (i.e. new bifascicular block) it is even more suspicious.
Below is “normal” RBBB:

Below is new RBBB with LAFB - 100% LAD occlusion:

In fact, new RBBB + LAFB is suggestive of a massive infarction (and poorer prognosis if not intervened on in a timely manner) because the LAD's septal perforators branch off proximally, so their involvement implies a proximal LAD occlusion. See diagrams below for some coronary artery anatomy (they are taken from an old blog post of mine).
Acute RBBB can also develop if the septum is stretched by acute RV strain (from massive PE).
A bit more on RBBB and STEMI...
Abnormal depolarisation should be followed by abnormal repolarisation - a principle known as “appropriate discordance.” If the QRS is predominantly upward, the ST-T segment should be downward, and vice versa. You might recognise this from the Sgarbossa criteria used to interpret ECGs in LBBB.
In RBBB, this principle applies to leads V1–V3, where the classic RSR' pattern is seen. In “normal” RBBB, these leads should show mild ST depression and inverted T waves (i.e. appropriate discordance).
A STEMI can manifest as “inappropriate concordance” in leads V1-V3. As the QRS is upward in these leads in RBBB, you can see concordant ST elevation. Another red flag for ischaemia is T wave “pseundonormalisation” in V1-V3 (that is, upright T waves where you’d normally expect them to be inverted).
Below is an an example of new RBBB/LAFB with concordant ST elevation in V2. 100% LAD occlusion:
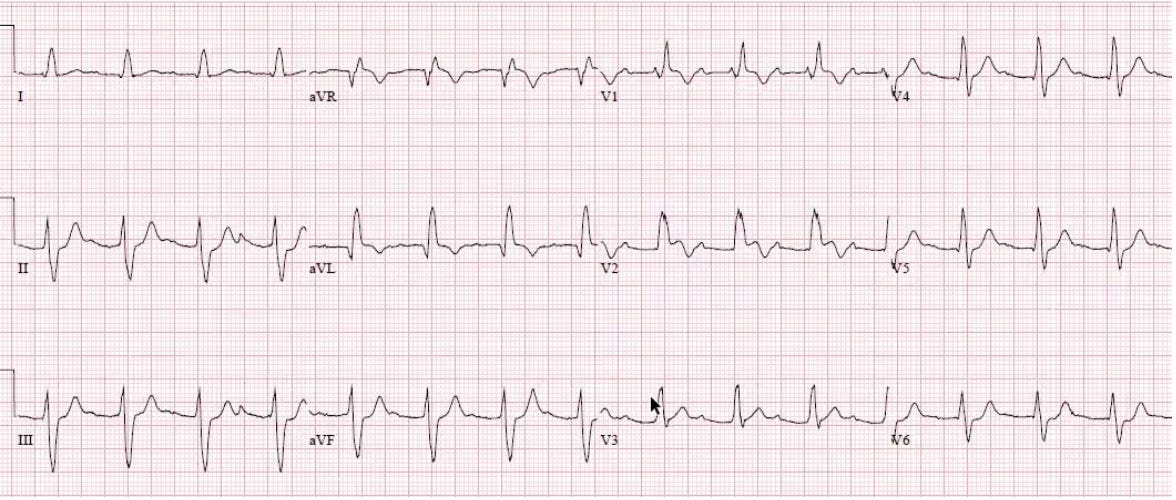
All other leads in RBBB won’t have the repolarisation abnormalities. Therefore, in the correct clinical context, ST elevation in any lead in RBBB is suggestive of STEMI.
I have taken the above ECGs from two blog posts worth reading from LITFL and Emergency Medicine Cases.
Cheers all,
Robbie